
Two armies at war can reach a stalemate, with both sides divided by sturdy fortress walls or a stretch of no man’s land. Similarly, battles between our immune cells and invading tuberculosis (TB)-causing bacteria, such as Mycobacterium tuberculosis, often form tuberculous granulomas: long-lasting, capsule-like structures that isolate the bacteria within the body.
“Granulomas are like a walled city built by our immune system and TB-causing bacteria as a compromise, where the body lets TB do what it wants inside those walls,” explained Stefan Oehlers, a Principal Investigator at the A*STAR Infectious Diseases Labs (A*STAR IDL).
Though TB can be effectively treated by antibiotics, their granulomas can persist in the lungs and result in subclinical or asymptomatic TB. Notably, granulomas could also make patients more prone to infection by other invaders: non-tuberculous mycobacteria (NTM) such as Mycobacterium abscessus.
“Around 25 percent of patients with NTM infections in Singapore and the region have a recent TB diagnosis. Singapore’s elderly are also a major demographic risk group for NTM infection, as they were endemically infected with TB decades ago,” said Oehlers. “As antibiotics against TB usually don’t work against NTM, we need to do everything we can to prevent infections by the latter.”
While previous studies and clinical reports have observed NTM residing in granulomas, it’s been unclear how exactly TB granulomas promote NTM infections. To shed more light on this relationship, an A*STAR IDL research team including Oehlers and Senior Principal Investigator Amit Singhal took a closer look at zebrafish infected with a fluorescent strain of Mycobacterium marinum—a human TB-like bacteria—which were then infected by similarly fluorescent M. abscessus.
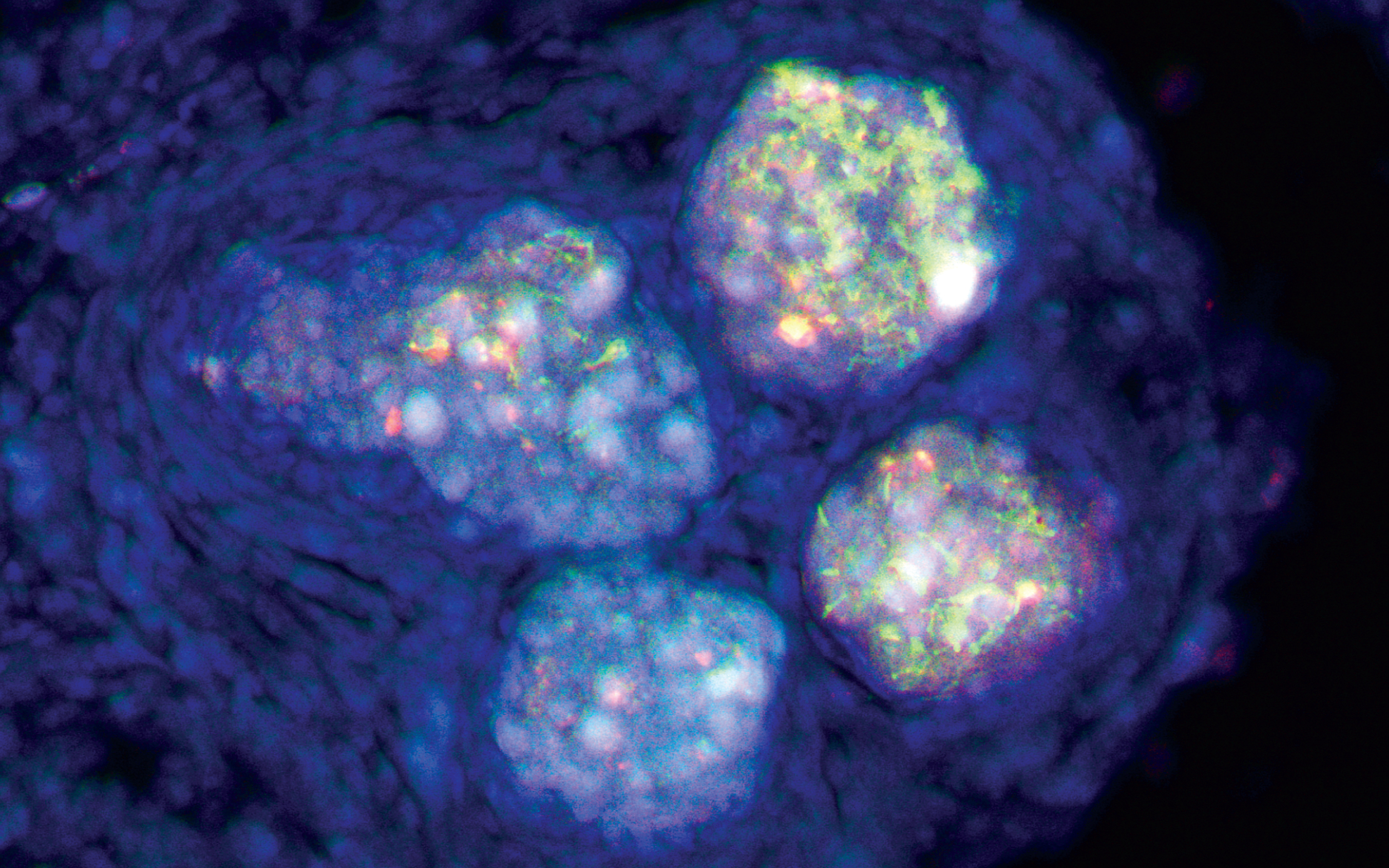
“Our ‘Eureka’ moment came when we first performed timelapse imaging and recorded M. abscessus streaming into a tuberculous granuloma,” said Oehlers.
From that one short movie, the team made two striking observations: the pre-existing granuloma fed the NTM, which rapidly grew in real time. The granuloma also sheltered the NTM from the immune system—by the end of the recording, most NTM that failed to reach the granuloma had been destroyed by immune cells.
The team then compared the gene expression patterns of M. abscessus grown in the zebrafish infection model with M. abscessus grown in culture media. They observed that bacteria from the model had more upregulated lipid metabolism, which suggested NTMs fuel their growth by feeding on caseum: the lipid-rich cell debris at the core of TB granulomas ‘left overs’ of the TB-causing bacteria. The scientists confirmed this when they saw M. abscessus grow rapidly in media with caseum.
Oehlers highlighted that these findings have implications for patients initially diagnosed with TB and NTM, but primarily treated for TB. “We need to think about monitoring and adaptably treating co-infection with antibiotics effective against both types of bugs,” said Oehlers.
The team plans to validate their findings by studying the links between unhealed granulomas—as indicated by exit X-rays of patients who completed TB treatment—with subsequent secondary NTM infections. “While this won’t immediately help at-risk patients, we think exit X-rays could be used to flag out the patients at the most risk of secondary infections early, when the infections will be the most curable,” Oehlers added.
The A*STAR-affiliated researchers contributing to this research are from the A*STAR Infectious Diseases Labs (A*STAR IDL).





